The Hard Problem Of Psychedelic Exceptionalism
Doxastic vulnerability, harmful belief change, and recovered memories

I. The Polarities of Psychedelic Exceptionalism
A lot of ink has been spilled over the past several decades to de-exceptionalize psychedelics. For much of that time, serious psychedelic researchers have been busy challenging negative exceptionalists—the Uncle Rays of the world who’d be more than happy to maintain a moratorium on psychedelic research and clinical applications. Over the last thirty years, psychedelic scientists have made a long march through the academy, investigating psychedelic treatments empirically and legitimizing them to some degree in the eyes of institutional gatekeepers (e.g., the FDA, the NIH/NIMH/NIDA, academic medical centers, psychiatry departments, VA hospitals, and major medical journals).
But in recent years, these psychedelic researchers have also had to face a different form of psychedelic exceptionalism. These are the positive psychedelic exceptionalists, who collectively form an increasingly influential and vocal group within the psychedelic world. After spending years and years hearing about “The promise of psychedelics for treating [insert bad thing],” these folks are—quite understandably—getting more than a little frustrated and impatient by the pace of play. “Enough of these multi-year clinical research trials!” they cry. “We already know, because we’ve already done the first-person science: psychedelics are the answer to [insert bad thing]! People have been suffering, languishing in the midst of a profoundly sick modern culture. We already have the antidote to our psychological, social, and civilizational problems, and now is the time to throw open the doors of perception en masse! Let’s just ram this through the FDA and be done with it! Bring these plant medicines to the world!”
All this is to say: there’s a lot of scrutiny, hope, and hype around psychedelic treatments right now. And psychedelic science accordingly finds itself balancing, sometimes precariously, between these two poles of psychedelic exceptionalism, forced on the one hand to dispel the remnant fears of negative exceptionalism, and on the other to variously cajole, reassure, or placate the positive exceptionalists who want these treatments to simply get off the ground by any means necessary.
The positive and negative psychedelic exceptionalists are, for the most part, diametrically opposed to each other. But if you take a step back here, you’ll notice that they both agree on something fundamental: both camps believe, in so many words, that the normal bioethical principles and scientific standards simply don’t apply to psychedelic treatments. They agree, in other words, that psychedelics are… exceptional.
But somewhat sequestered from the hype and hysteria, there’s a more nuanced form of this same debate taking place within academic corners of the psychedelic world—at conferences, lab meetings, and in peer-reviewed back-and-forths. So far, this has played out as an academic debate, which usually means it gets mostly ignored by the wider world. But I think this one is fairly unignorable. The United States will probably approve its first psychedelic treatment within the next twelve months. Compass Pathways has completed its Phase 3 trials of synthetic psilocybin for treatment-resistant depression and expects to finish its FDA application by the end of 2026, with a decision possible in early 2027. Other psychedelic biotech companies and nonprofits are close behind in a horse race that has been further accelerated—for better or worse—by Trump’s recent executive order. This means that the rules and policies governing classic psychedelic treatments are about to get written at the federal level for the first time, and these kinds of rules can be slow to rewrite.
Accordingly, I wanted to take a critical look at the core questions of psychedelic exceptionalism: In what ways, if any, are these treatments unlike anything that has come before them in medicine? In what follows, I’ll attempt to answer these questions, and then highlight some issues I unearthed through this deep dive that I think are worth taking seriously by regulators, scientists, practitioners, prospective patients, and anyone else who cares about how this whole thing goes.
II. The Varieties of Psychedelic Exceptionalism
The academic version of this debate picks up as a special issue on psychedelic ethics in The American Journal of Bioethics. There, legal scholars Cohen and Marks argued that—fearmongering and hype cycles aside—psychedelics really are exceptional in at least some ethical respects that need to be reckoned with. To this, Cheung and colleagues countered that while psychedelics may be ethically distinctive, they are not truly exceptional; it is fully possible—they argued—to leverage the same longstanding bioethical principles (namely, autonomy, beneficence, nonmaleficence, and justice) and pre-existing clinical protocols to facilitate the integration of psychedelic treatments into mainstream biomedicine.
A slew of commentaries followed, including one by philosopher Daniel Villiger, who distinguished between two claims that often get conflated in this discussion: standards exceptionalism, which holds that psychedelic treatments are so unique that they should be judged by different ethical and evidentiary standards than other treatments, and policy exceptionalism, which holds that while psychedelic treatments should be judged by the same standards as any other therapeutic treatment, these treatments are so unique that meeting said standards will require novel protocols and regulatory structures that are not found anywhere else in modern medicine.1
Standards exceptionalism: psychedelic treatments are so unique that they should be judged by different ethical and evidentiary standards than other treatments.
Policy exceptionalism: while psychedelic treatments should be judged by the same standards as any other therapeutic treatment, these treatments are so unique that meeting said standards will require novel protocols and regulatory structures that are not found anywhere else in modern medicine.
Once this distinction was made, everyone in the debate promptly agreed that standards exceptionalism was pretty indefensible. All agreed, in other words, that psychedelic treatments should be subject to the same evidentiary burdens, risk-benefit calculus, and regulatory scrutiny as any other clinical intervention. After all, we already have effective bioethical principles2 that capture the relevant concerns: patient safety, informed consent, clinical benefit, therapist conduct, iatrogenic harm, et cetera.
As for how we empirically test the clinical efficacy of psychedelic treatments, it also seems like a mistake to lower the bar because a molecule is marketed as sacred or has a long history of use by certain indigenous communities.3 And on the flip side, it also seems wrong to raise the bar simply because a drug bears countercultural baggage.
Therefore, the crux of the debate hinges on whether or not psychedelics are policy exceptional—whether these treatments are so unique that meeting said standards will require novel protocols and regulatory structures that modern medicine has never developed before. Call this the hard problem of psychedelic exceptionalism, where the debate is still live.
III. The Hard Problem of Psychedelic Exceptionalism
Before going further with the academic debate, let’s make the stakes feel more real here:
Seriously, how do you regulate a treatment approach that fuses a controlled substance with hours of psychotherapy, whose effects hinge on expectations and surroundings, and which regularly brings on not just emotional catharsis but also experiences of “ego death,” “self-transcendence,” and “unitive consciousness”? How do you regulate a treatment that puts people into a highly suggestible and emotionally vulnerable state, gives them one of the most personally and spiritually meaningful experiences of their lives, and then may leave them with enduring and broad-based changes to their beliefs and worldviews? Psychedelic treatments are, at the very least, profoundly distinctive—quite different in important respects than any other therapeutic in the modern clinical arsenal.
The live question of policy exceptionalism is then: do psychedelic treatments require clinical protocols for safe administration that no other medical treatment needs?
Pause here, and take a moment to seriously consider that question.
What do you think?

If you’re like many (myself included), your first intuition will be something like:
Absolutely, yes.
After all, psychedelics are nothing like psychiatric medications you can just pick up at a pharmacy; psychedelic treatments put patients in a state of psychological and physical vulnerability vis-à-vis the monitoring provider in the room, and there should obviously be strong safeguards here to ensure patient safety. To motivate this further, consider that there have been several widely discussed instances of gross provider misconduct—inappropriate touching, boundary violations, and unusual therapist-patient intimacy during or after dosing sessions. Shouldn’t this be a knock-down argument in favor of policy exceptionalism?
Not so fast. The question is not whether these violations are morally horrifying (they are), but whether they are truly unique to psychedelic treatments. In fact, the risk of such abuse is present to some degree during standard talk therapy, as well as when patients are put under general anesthesia. The key point here is that because these same risks exist to some degree in other treatments, the risk-mitigation protocols applied to these other treatments give us pre-existing templates we can then repurpose for the context of psychedelic psychotherapy. So, contra policy exceptionalism, we would not need completely new policies to address the issues surrounding therapeutic touch.4
So, what would it take for psychedelic treatments to be truly exceptional at the level of policy? At this point, the debate can get somewhat hard to follow, so here’s a graphic you can refer back to if you get lost:
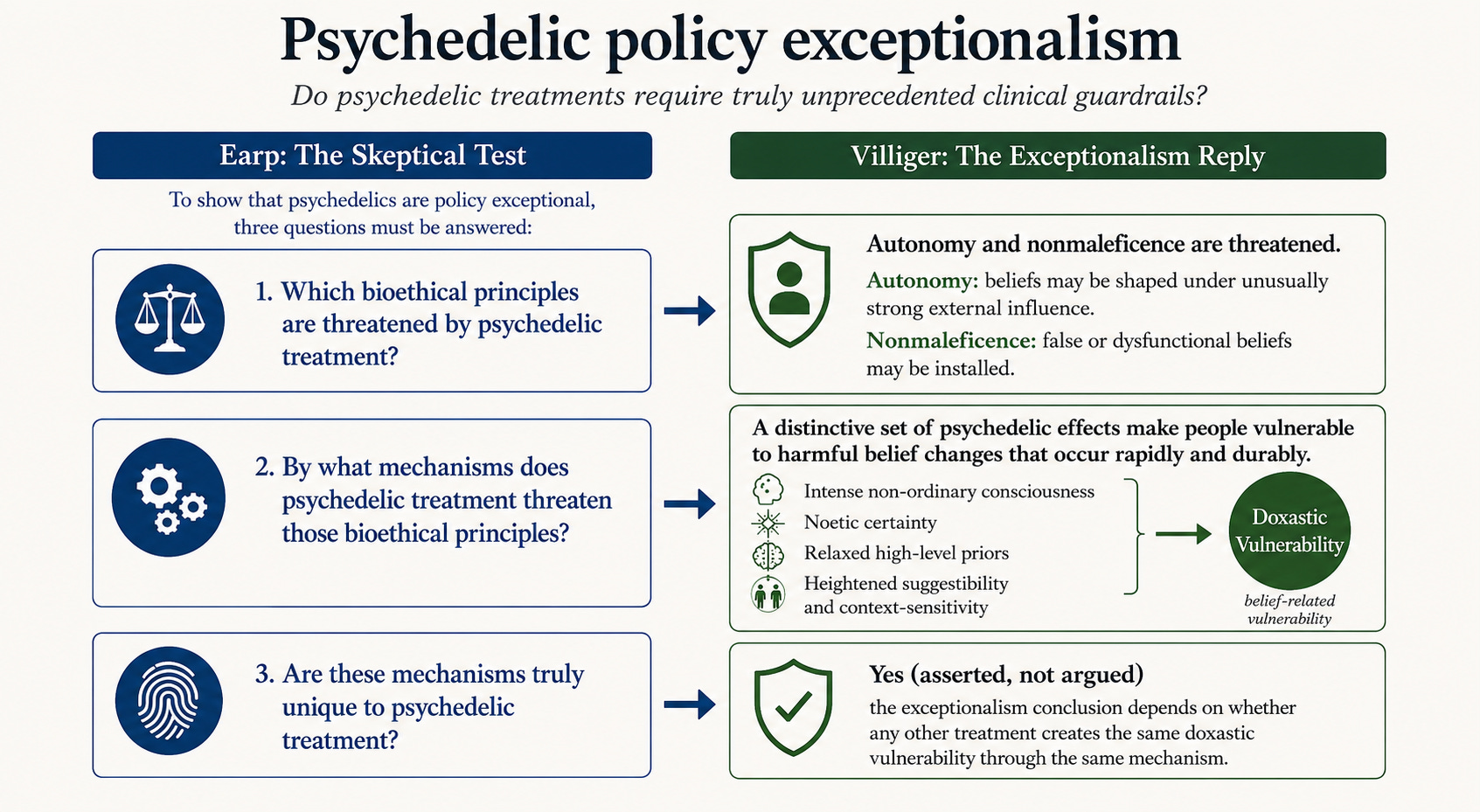
Earp and colleagues voice skepticism, arguing that the risks of psychedelic treatments are neither truly unique nor necessitate the development of truly novel guardrails that the medical world has never seen before. These authors then identify three criteria that must be met for psychedelics to be considered policy exceptional by their lights:
Identify the specific bioethical principle that is threatened by psychedelic treatment
Identify the mechanisms by which psychedelic treatment threatens that principle
Show that no other treatment in our therapeutic arsenal threatens the same principle via the same mechanism
This three-part test corresponds to the left-hand side of the graphic.
In response, Villiger, still defending policy exceptionalism, points to several features of the psychedelic experience that are meaningfully unique. Specifically, psychedelic experiences:
Taken together, these features of the psychedelic experience can place individuals in a condition of unusual doxastic vulnerability—that is, vulnerability with respect to what they come to believe (“doxastic” is just a fancy term for “belief-related”). In plainer terms, psychedelics can make people highly receptive to sweeping and rapid revisions in how they understand themselves, other people, their past, and the world at large.
Villiger argues that heightened doxastic vulnerability can threaten both patient autonomy (e.g., because a belief arrived at under heavy external influence isn’t fully one’s own), as well as the principle of clinical nonmaleficence (i.e., “first, do not harm”)—some of the beliefs that get installed may be either incorrect or highly dysfunctional.
Lastly, Villiger asserts (though doesn’t spend much time arguing for) the claim that no other intervention in mainstream mental or physical health makes patients doxastically vulnerable in a meaningfully similar way.
So, at the end of the day, Villiger concludes that psychedelic treatments are policy exceptional, and that we should therefore get to work crafting exceptional policies to reduce the risk of rapid, enduring, harmful belief change.
IV. Wait… What Kinds of Belief Change Are We Even Talking About Here?
So far, we have been talking a lot about doxastic vulnerability in the abstract. It would be helpful at this stage to get more concrete about the specific belief changes that might meaningfully be said to harm psychedelic therapy patients. After all, not all belief change is for the worse. Psychedelic therapy is a mental health treatment, so we’d expect and want a patient’s beliefs to change insofar as doing so also eliminates unnecessary psychological suffering.
What then are the truly harmful beliefs that psychedelics might install?
Metaphysical and Normative Beliefs
Start with what’s generally the least concerning category: metaphysical and normative belief change. Psychedelics often seem to leave people with large, global convictions about consciousness, divinity, love, nature, death, or the moral structure of the universe. Some of these changes may be salutary; indeed, many of the most common psychedelic “insights” are hard not to like. It is not exactly a public health crisis if someone comes away believing that life is precious, consciousness is more mysterious than they thought, or that human beings ought to be kinder to one another. Still, these are not ordinary symptom-focused therapeutic revisions. They are often broad, emotionally charged, and difficult to adjudicate, because the claims themselves are frequently metaphysical or normative rather than empirical. “Everything is connected,” “love is the highest good,” and “consciousness pervades reality” are not the kinds of propositions one can easily test against the world. So even when the resulting beliefs are benign or beautiful, they raise a real autonomy concern: a person may come to hold unusually large, life-orienting beliefs with a degree of certainty that outruns the available evidence.
 by Alex Grey | Artsy")
Again, this is mostly benign, or even therapeutic. But while rare, there are also cases where psychedelics have caused people’s metaphysical beliefs to change in a straightforwardly harmful way. In one case, an airline pilot took mushrooms, which caused him to believe that his normal, waking reality was only a dream. Two days later, he attempted to shut off a plane’s engines mid-flight to wake himself up (luckily, no one was harmed). Of course, this is only a single case, and one that arose from recreational use outside a clinical context. Had the pilot taken psychedelics in a clinical setting, a competent practitioner could have identified this derealization before it became a serious safety issue. And to be clear, extended derealization of this sort is a very rare occurrence after a psychedelic experience. Still, this case serves as a useful reminder that our fundamental beliefs about the world shape our actions, and that pharmacologically reshuffling these beliefs too radically and too quickly can have serious consequences.
Grandiose Beliefs
But even though I’m writing this section at 33,000 feet, I’m less worried about how psychedelics change our view of the universe than I am about how we then come to see our place in it. In particular, certain metaphysical beliefs occasioned by psychedelics (e.g., “everything is divine”; “everything is godlike”) can easily shade into beliefs that confer a grandiose sense of specialness (e.g., “I am divine”; “I am godlike”). In some spiritual traditions, claims of this general form can be metabolized in disciplined, non-grandiose ways. But to the Western mind, these experiences can sometimes slide into messianic self-understanding, spiritual narcissism, or the conviction that one’s post-trip intuitions should override the concerns of friends, family, clinicians, or basic prudence.

If psychedelics can relax prior beliefs, intensify felt significance, and generate noetic certainty, then they can sometimes amplify the ego, even under the guise of dissolving it. Again, like extended derealization, spiritual narcissism of this sort is not at all a common outcome of psychedelic use. But these cases have occurred, with predictably catastrophic effects.
Beliefs About Past Trauma and Recovered Memory Experiences
But for me, the most clinically concerning category of belief change comes in the form not of altered metaphysics or ethics, but an altered sense of the past. There are multiple case reports of people who claim to have recovered memories of previously forgotten events—including child abuse—during psychedelic experiences.
These experiences often arrive with the felt quality of a vivid, embodied revelation, and may be accompanied by the deep sense that something long hidden has finally been disclosed. A recovered memory experience may feel less like “maybe this happened” than “now I finally know what happened.”
Yet despite the first-person feelings of certainty that these experiences can involve, the wider psychedelic world is sharply divided on how to interpret these phenomena. Some view these recovered memory experiences as an essential part of emotional healing. Per this “Body Keeps the Score” view, psychedelics act as psychic solvents that unlock buried memories of real, deeply painful autobiographical events, so that they can be emotionally processed and moved through. Others see these experiences as emotional and symbolic confabulations of a mind in the midst of a highly altered state. It is not hard to see how such experiences could be occasioned by the mechanisms we’ve touched on above. If psychedelics relax high-level priors, intensify felt significance, heighten suggestibility, and generate noetic certainty, then ambiguous images, bodily sensations, fragments of fear, sexual feelings, dreams, or therapeutic cues may be organized into a newly coherent autobiographical story.
Psychedelic recovered memory experiences are not a recent phenomenon. These experiences were first documented in the 1950s, and have occurred in multiple recent trials of psychedelic therapy. In one open trial of psilocybin for anorexia nervosa, two out of the ten trial participants reported recovered memory experiences during treatment. And outside the research world, psychedelic recovered memory experiences have also inspired several memoirs. One such recently published memoir, Alex Abraham’s Trauma and Ecstasy: How Psychedelics Made My Life Worth Living, illustrates just how high the stakes can become here. Abraham documents how he entered psychedelic therapy seeking relief from unexplained sexual and pelvic symptoms, only later coming to understand his suffering through the framework of forgotten childhood sexual abuse; over multiple sessions of psychedelic therapy with different facilitators, Abraham describes increasingly violent somatic reactions, dreams of being raped as a child, a wholesale reorganization of his relationship to his parents, and eventual efforts to pursue justice against the alleged abuser, a former grade-school music teacher.
It is well beyond my scope or ability to adjudicate the factual veracity of this or any other psychedelic recovered memory experience. That’s not my aim. But I think it’s important in the first place to raise the issue. These experiences are both extremely significant clinical events and highly underemphasized in psychedelic science. I hope to touch more on this topic in the future, and also raise a concern as to why these experiences might have gone underemphasized even by some of the most careful and rigorous researchers in psychedelic science.
V. Conclusion
Bringing us back to the question that motivated all this: Are psychedelic treatments exceptional? I have the same obvious, boring, antiviral answer I find myself giving to most questions I tackle here: it’s complicated. Psychedelic treatments are not standards exceptional; they aren’t exceptional in the sense that we should raise or lower our ethical or evidentiary standards when weighing their effectiveness. But these treatments do involve real doxastic vulnerabilities, which can lead—albeit rarely—to very bad outcomes. At minimum, these treatments will require thoughtful policies and safeguards.
Whether those policies need to be built from scratch, or can be retrofitted from protocols elsewhere in medicine, is the still live, still open question of policy exceptionalism. A satisfying answer requires the field to explore other clinical treatments that carry a similar risk profiles, and then ask how well prior safeguards actually worked historically, and how effectively they can be retrofit to psychedelic treatment contexts.
Of all the risks we’ve surveyed, the one I keep returning to is the issue of recovered memory experiences. This is an area where not just the clinical but also the legal stakes are high, and where the potential for harm is least contained by good intentions. As FDA approval approaches, the question is no longer hypothetical: either we install meaningful safeguards now, or we get the Memory Wars, Part 2—this time with psychedelics.

Villiger calls this “Type A” and “Type B” exceptionalism, respectively.
Namely:
Autonomy: patients should be able to make informed, voluntary decisions about whether to undergo treatment, without being coerced, manipulated, or swept along by therapist enthusiasm, cultural hype, or their own impaired state during the intervention.
Beneficence: clinicians and researchers should aim to provide real therapeutic benefit, not merely intense, meaningful, or spiritually impressive experiences that may or may not translate into durable clinical improvement.
Nonmaleficence: clinicians and researchers should take seriously the possibility of harm, including not only ordinary adverse events, but also more distinctive risks such as destabilization, dependency on the therapist, iatrogenic belief change, false insight, and recovered memory experiences.
Justice: access, burdens, risks, and benefits should be distributed fairly, rather than allowing psychedelic medicine to become a boutique treatment for the affluent, an exploitative research frontier for vulnerable populations, or a culturally extractive industry built on Indigenous practices without meaningful reciprocity.
If you don’t think this is sufficiently sympathetic to the cause of psychedelic therapy, ask yourself this: If these treatments really do work, wouldn’t we expect them to work well enough to clear the scientific and ethical hurdles that we set for every other treatment? And wouldn’t lowering or otherwise changing the standards for psychedelic treatments ultimately be counterproductive from a dissemination perspective? Wouldn’t this just reduce the credibility of these treatments in the eyes of the wider world?
To be clear though, the issue of touch in psychedelic therapy is still a live and important discussion, and not one I’m going to be able to do justice to here. For a lot more careful discussion on best practices concerning the use of therapeutic touch in psychedelic psychotherapy, see Neitzke-Spruill et al., Yang, Insua-Summerhays & Jacobs, and Luoma & LeJeune. Feel free to shoot me a private message if you have trouble accessing any of these articles.