Psilocybin Facilitation Is Probably Not a Viable Standalone Career
Would-be psychedelic practitioners should seriously consider also getting licensed as a standard mental healthcare provider

I’m going through the didactic trainings to become a psilocybin facilitator1 right now, and I have a lot of thoughts about it. One thing I’ve noticed is that the people I’m training with come from a LOT of different backgrounds. The people in my program include therapists and nurse practitioners, as well as breathwork practitioners, wellness coaches, and psychedelic facilitators who have worked for years/decades in the “psychedelic underground.” There are also a couple of people who have no prior experience in any wellness service: former customer service professionals and former exotic dancers who are making a career pivot.
It’s been becoming increasingly clear to me that people in these latter groups—by which I mean people without a license to provide some form of mental health treatment—will have quite a difficult time carving out a viable career in psychedelic practice.
It’s worth spelling out precisely why this is the case, and what that means for people trying to go into this nascent field.
The Meditation Teacher Problem
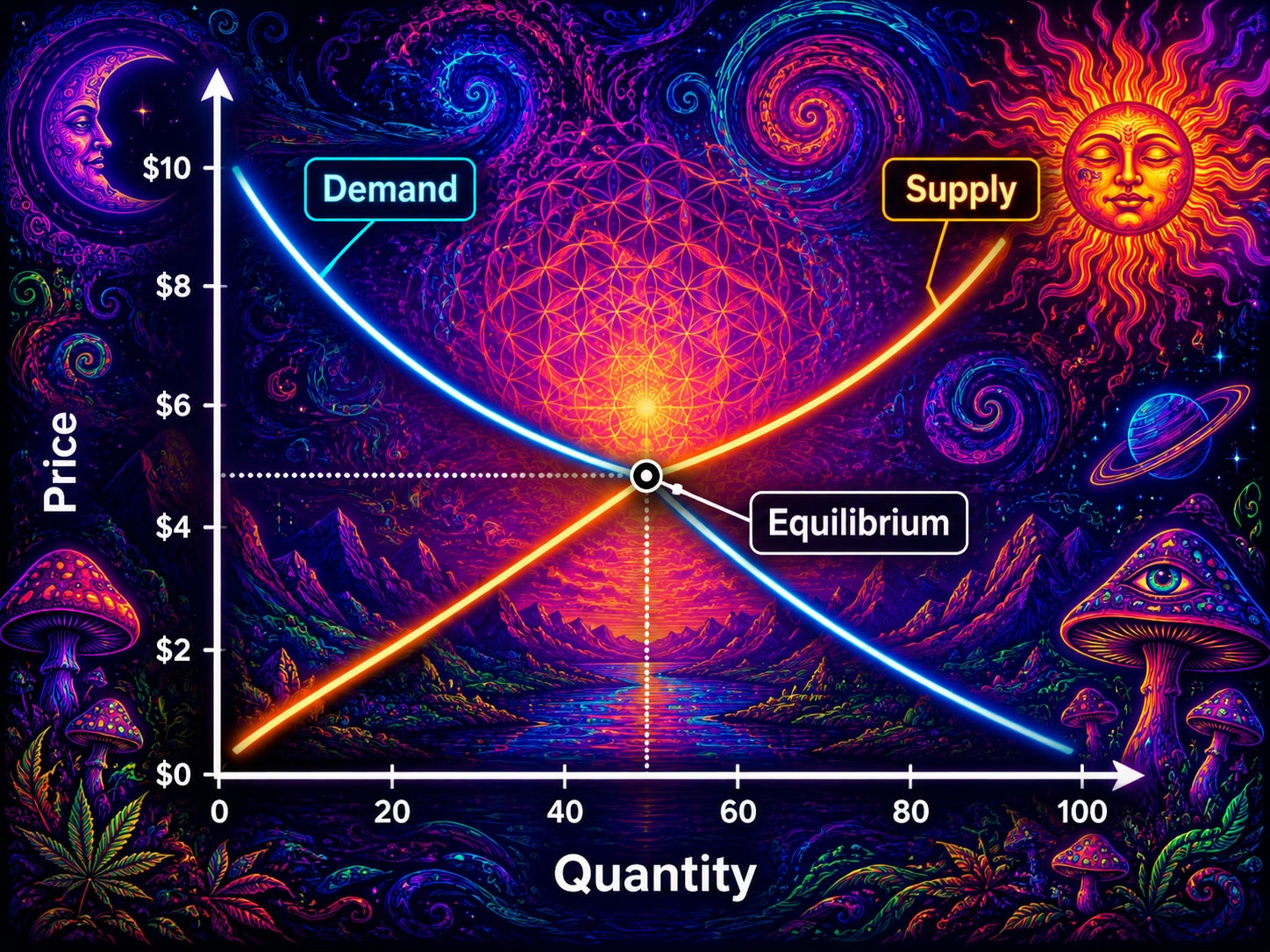
The first (boring? obvious?) structural issue is that, per the frank admission of people currently in the space, there is an absolute glut of psilocybin facilitators in Oregon and Colorado. There are more facilitators than there are people seeking facilitation, at least at prices that make the whole enterprise at all economically viable for an individual facilitator. Add in the fact that psilocybin facilitation can’t be billed to insurance, and you have a really hard market for this service.
Earlier today, I got coffee with the owner of a psilocybin services practice, who has been in the field for the past three years.2 When I asked him about the supply-demand problem, he gave me an interesting analogy I’ve been thinking through:
Becoming a psilocybin facilitator in Oregon or Colorado today is a lot like becoming a meditation teacher. There are very many of them. Many are wise, intuitive, kind, and well-meaning, although you also have some who are probably too far out there for their own (or anyone’s) good. A small number have more clients than they can handle. A meaningful subset are also licensed clinicians. And for ninety-five percent of them, the work is something they do on a very part-time basis, with the help of a financially supportive spouse or unrelated day job.
This struck me as essentially correct, and it raises an uncomfortable truth: psychedelic facilitation is often marketed by psilocybin training programs as a viable career path, but functions more like a hobby or side gig for most actual facilitators. From a purely financial perspective (of course, not the only valid perspective), the costs of facilitator training—around $7,000 and 4-to-6 months—are tough to square with the economic realities of the field as it currently stands.

Further Professional Considerations
Most people in the field already know the above. But in talking to practicing psilocybin facilitators, I’ve realized there are some additional issues at play. Some of these are downstream of the basic supply-demand issue, but are worth identifying separately:
Facilitation referral networks favor mental health professionals. It sounds like one major client referral pipeline runs through physicians and licensed mental health providers. Rightly or wrongly (and I think mostly rightly, given the fact that most people seeking out psilocybin services are doing so with explicit mental health goals in mind), those referrers are more likely to send patients to facilitators with clinical credentials. When there are ten possible facilitators, and one with a clinical license, you might as well refer to the one with the clinical license, all else equal.
Many clients want the benefits without the woo. Many would-be clients have heard that psychedelics could be really psychologically healing and want that for themselves, but also don’t want to have their entire spiritual and metaphysical worldviews upended in the process. That is, they just want to feel better; they don’t actually want the hippie-style, Burning Man aesthetics and “we are but fragments of the Divine smiling back at each other” thing. This is very reasonable. Because of their training in standard therapy as usual, clinicians—even those with a wookish bent—can more authentically dial it back and keep the aesthetic sanitized and somewhat mid-century therapeutic modern.
A dual clinical license and psychedelic facilitation license differentiates you in two worlds. A clinical license is a strong differentiator inside the psychedelic space, in that you can claim a target population (e.g., “I work with treatment-resistant depression, with and without psychedelics”) rather than just a modality (”I do psilocybin facilitation” [yes, so does every facilitator]). And the reverse holds in mainstream therapy circles, where psychedelic specialization is a real niche. Facilitators without a clinical license get neither side of this: they have a harder time to credibly claim a population, and no foothold in the broader therapy world to begin with.
No fallback if the field stalls. Oregon’s program is not financially self-sustaining at current volumes; Colorado’s program is barely out of the gate. State-regulated psilocybin could remain a small, expensive boutique service indefinitely, or it could contract under a less friendly political administration. If you have committed to facilitation as your career, your downside scenario is the field shrinking around you while you watch.
No fallback even if the field succeeds. Suppose the optimistic scenario happens: federal rescheduling, insurance reimbursement, and mainstream adoption of psychedelic-assisted therapy. The economics that follow are not friendly to the independent facilitator without other credentials. Insurance pays licensed providers. Integrated medical groups and chains will dominate the high-volume end. Prices come down, margins compress, and the field will professionalize in the boring way every field eventually professionalizes. The people who do well in that world are the people with a license to prescribe and to bill health insurance. Absent that, you’re looking even in the best-case scenario at a vocation where you’re employed by a larger center or network, which takes away a good deal of professional autonomy and reduces your comp.
My Recommendation
If you are just starting out in this field—maybe still in college or looking to pivot into psychedelic practice—the single biggest piece of advice I can offer: get a regular mental health practitioner license. LCSW, LPC, LMFT, psychiatric nurse practitioner, PhD, MD/DO.3 Pick one and go. Then let the craft of ordinary practice be the firm baseline on which to build the vocational stability and professional expertise that then allow you to aim high. Psychedelic-assisted therapy is best conceptualized here as the passion project and the higher heights that you’re ultimately aiming for, but not the sole basis on which to build a working life.
Objections, Counters, and Caveats
First, a caveat: I am describing where the field is and where I think it will go over the next decade or so; I could be totally off here. I am not describing where I think the field should be or should be going; that’s not part of the story here.4
One objection goes something like:
Of COURSE you’d say this! You’re getting a mental health license yourself, and you’d LOVE it if fewer people crowded the field! But you can’t fool me!
🍄😎🍄
I would invite you to look at my actual incentive structure here. Precisely because I went for a traditional mental health professional license, my professional path does not depend heavily on the health of the psychedelic field. If state-regulated psilocybin services vanished entirely, my professional life would be approximately unchanged; I would eat some training-related sunk costs, but I would just find another way to help people. But those whose financial futures ARE determined by the future of this field—the people who run facilitator training programs, the facilitators without other licenses, the consultants and conference organizers and entrepreneurs selling psychedelic supplements and the like—these are the people whose advice on whether to enter the field SHOULD be treated with the most suspicion.
This is just the ordinary move of asking: “Who profits from your decision to do the thing they’re recommending?” It is not a novel epistemic principle. I mention it only because the psychedelic space, with its standing emphasis on openness, trust, authenticity, and communalism, has an unusual ability to make questions like this feel rude. But it’s actually not rude to think about incentives; it’s extremely sensible.
Actually, the strongest counterargument to my recommendation concerns how this advice might affect the psychedelic field as a whole. Because I am, in effect, recommending that folks spend years and real money becoming a particular kind of credentialed professional—one whose training is shaped by managed care, DSM-5 epistemology, and a guild structure that has been historically hostile to exactly the practices that make psychedelic work valuable in the first place. The underground facilitators with twenty years of sitting experience know things my graduate program did not teach me and arguably cannot teach me, and the cultural and spiritual lineages they draw on are not interchangeable with a CBT manual. There is a real sense in which “just get licensed” is the kind of advice that, taken collectively, would hollow out the field’s most distinctive features and replace them with a sanitized clinical version that bills at $250/hour and uses the word “embodiment” twice per session.
That’s all worth taking seriously. My argument is narrower: it’s not that the licensed path produces better facilitators (often it does not), but that it produces facilitators who can pay rent. And crucially, facilitators who can pay rent are ones who have more autonomy, voice, and the standing to call out grift when they see it without losing their livelihoods. Without this widespread autonomy, the psychedelic field runs on vibes and hype, and pervasive ethical issues get swept under the table.
How to Change a Clinical Culture
While we’re zoomed out here, consider the good you could do within a given culture versus outside of it. The psychedelic practice landscape is full of self-styled renegades and independent thinkers (how else would one come to this field if not by ignoring the categorical drug prohibitionism that they teach you in 9th grade health class?) So it may be more comfortable for these personalities to sit outside of larger institutions, build their own practices, et cetera.
But here’s the thing: if part of your broader “why” in getting into this field is to actually change the way our culture handles psychological suffering and healing (worthy aim), you will probably be in a better position to effect that change from the inside the current clinical structures and guilds that we have today; if the MAPS/Lykos FDA approval process showed us anything, it’s that it’s hard to make real societal change from the playa or the woods. Some aspects of psychedelic culture—the person-centeredness, the openness to spirituality, the emphasis on embodiment—are sorely needed in a world of managed care and unending clinical acronyms. Put differently, you can either sit around in a campfire with likeminded psychedelicists, agreeing with each other about how every facet of modern clinical practice is poison, or you can take a stand in a clinical supervision group, where you might actually have the power to change hearts and minds, and eventually move the clinical mainstream a couple steps closer to the fire.
The former is the path of least resistance, but perhaps the latter is the path of more growth, both for yourself and for the field.
Am I off base here? Too Pollyanna? Too cynical? Both?
Let me know:
Some context: I’m currently living in Oregon—one of the two states in the country (the other being Colorado) where one can legally take psilocybin in facilitated sessions. While things are moving fast in the psychedelic field, psychedelic-assisted therapy as such is not yet something that a licensed mental health clinician can legally provide. Instead (for now) “psilocybin facilitation” exists as a separate state-licensed profession, with its own training programs, its own scope of practice, and a regulatory framework that conspicuously avoids the word “therapy,” for better or worse.
Three years being, roughly, the entire history of legal psilocybin services in Oregon. So: a veteran.
Actually, the specific path actually matters a lot, but that’s not the point of this post. Tl;dr, the nurse practitioner path seems like the juice here that’s most worth the squeeze. Also: please don’t pay $400K for a PsyD.
Though to put my cards on the table a bit: I do think anyone doing this work ought to have some training in standard psychotherapy, if only to understand the ethics and role-induction of a therapeutic encounter. It is wild that you can become a psilocybin facilitator with 4-6 months of 1/2x per week Zoom calls, plus a weekend-long practicum. Contrast that with the process of getting licensed to practice psychotherapy: two years of full-time coursework, plus 2,000-3,000 hours of supervised clinical work. No one in the psychedelic practice space will tell you that the facilitator training is too rigorous; it’s just an expensive rubber stamp, and that’s a serious issue.