Contra Contra CBT
How I Learned to Stop Worrying About CBT™ and Sort of Make Peace With cbt

I. Tales from the Thousand and One CBT-Critical Commentaries
There’s a kind of critical commentary on cognitive-behavioral therapy (CBT) that’s been flowering for at least the last two decades. Some classics of this genre (which I highly recommend) include Jonathan Shedler’s Where Is the Evidence for “Evidence-Based” Therapy and Scott Alexander’s CBT in the Water Supply.
I recently came across another such critique (also highly recommended) by Josh Zlatkus, a therapist and writer at Living Fossils. This essay is multi-pronged, covering many of the common CBT-critical beats, including:
CBT is wildly oversold by individuals and institutions with vested interests in its superiority vis-à-vis other therapeutic orientations.
But for all the hype, CBT doesn’t actually work any better than any other form of psychotherapy that has been empirically studied.1
CBT excessively gravitates towards short-term symptom reduction while missing on broader therapeutic aims (e.g., building a life worth living, subjective meaning- and sense-making). As such, CBT can flatten the human experience, eliminating subjectivity and nuance.
CBT rests on dubious assumptions regarding human nature, and doesn’t take evolutionary theory or developmental history seriously enough.
CBT’s aesthetics are simply lame.
Ouch! I want to be clear at the outset that these are important critiques worth taking seriously and wrestling with, particularly by CBT researchers and practitioners. All the above matters because CBT is increasingly regarded as the default therapy in American society, and it’s by far the most dominant theoretical orientation among therapist training programs.
I have firsthand experience dealing with this, having just come out of a clinical science training environment. I came into this program with a generally negative opinion of CBT, which was informed by both the critiques above and by my own forays into the orientation.
But to my dismay, the clinics I trained at and the supervision groups I attended were pretty much exclusively focused on CBT, broadly construed.2 These were contexts in which terms like “transference” and “unconscious” were verboten, and where “introject” and “disavowal” were simply unknown. I was frustrated, but because I was already locked into these training settings,3 I decided it would be more helpful to at least try to change the way I viewed CBT. So, over the next three years, I did everything I could to steelman this orientation and find ways to regard it in a good light.
In hindsight, many of the reframes I came to were complete and utter cope. But one in particular seems valid to me even now. So, while it’s still fresh, I want to give my strongest honest rehabilitation of CBT, explaining where I see this orientation usefully fitting into the broader world of psychotherapy.
The core of my argument is that CBT’s Achilles heel, the element that makes many therapists, clients, and critical thinkers recoil, is not so much its substance but its scientistic aesthetics. Inflated by its aesthetics, CBT risks simultaneously oversimplifying the complex, overcomplicating the simple, and generally overpromising. Unfortunately, the scientism isn’t something that can be easily separated from the core of CBT, as it was baked in from the outset for the sake of marketing. Further, the scientistic aesthetics are maintained by perverse incentives within academic psychology, where you can make an entire career and livelihood pushing out yet another CBT™ manual, workbook, or workshop.
But notwithstanding the scientistic aesthetics of CBT™, there is also a valuable substance here worth identifying, standing up for, and even championing—call it cbt. The single most valuable aspect of cbt is the cognitive model, which I’ll argue can serve as a sort of lingua franca or Rosetta Stone across therapeutic orientations, allowing practitioners to have a mutually-intelligible way of discussing their cases and how they navigate the therapeutic process. The cognitive model’s extreme simplicity and—critically—its interoperability with other therapeutic orientations is the single best reason to have cbt (but not CBT™) be among the first therapeutic orientations that training therapists learn.
II. The Frankly Abysmal Aesthetics of CBT™
I wrote 3,000 words on the frankly abysmal aesthetics of CBT™, which I’m not publishing here because (1) others covered this well enough, (2) my aim here is to be constructive, and (3) I’m using my real name on this platform while still working at predominantly CBT-oriented training environments.
So I’ll just let this CBT™ book speak for itself:

In this innovative book, Feeing (sic.) Great, Dr. Burns, describes a new and revolutionary high-speed treatment for depression and anxiety based on 40 years of research and more than 40,000 hours treating individuals with severe mood problems. The goal is not just a rapid and complete elimination of negative feelings, but the development of feelings of joy and enlightenment.
Dr. Burns will provide you with inspiring and mind-blowing case studies along with more than 50 amazing tools to crush the negative thoughts that rob you of happiness and self-esteem.
You can change the way you feel! You owe it to yourself to FEEL GREAT!
…This makes me feel the call of the void.
III. cbt as the Humble Bones of Treatment
Given 3,000 words of redacted material, what about CBT™ could possibly be worth saving? When it comes to the aesthetics, close to nothing. But when it comes to the theoretical architecture underneath (call it cbt), several things stand out.
First, two low hanging fruits to pick: There are obviously ways to do CBT without coming off like an eighth-grader at a science fair or a TEDx book merchant, even if doing so is like swimming against the current.
Second and more importantly, we really do need some degree of empiricism to check that what we’re doing in therapy actually works, and a culture that leans too far into scientism is at least failing in a more correctable direction than one that abandons measurement altogether.
But the thing that’s most worth broadcasting, and even championing about cbt is that the theory underlying it—the cognitive model—can, when used appropriately and with humility, be an extremely useful clinical tool. Let’s take a look at the cognitive model for a minute, in all its simplicity:
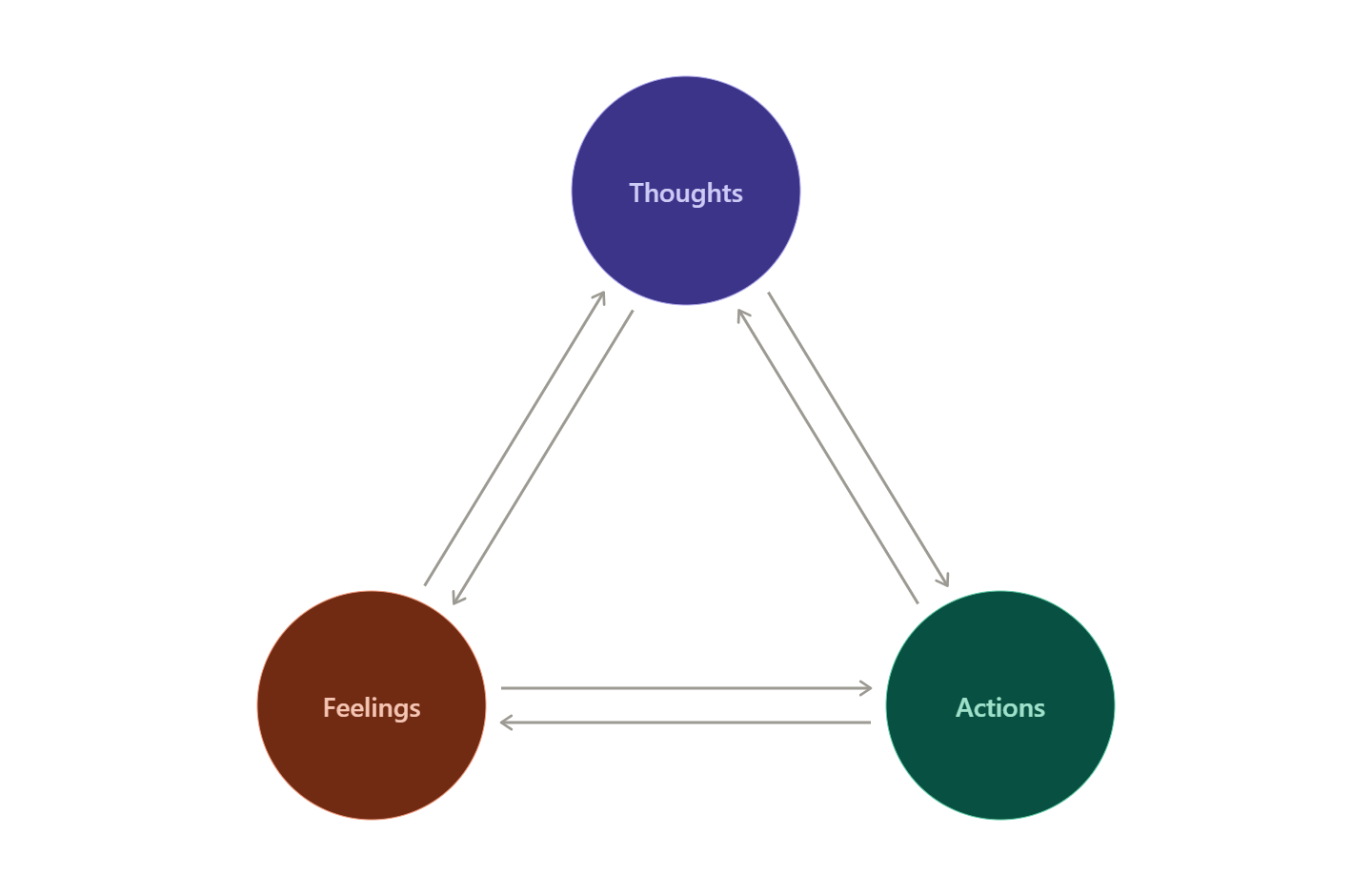
That’s it. The core starting point of cbt is nothing more or less than the extremely basic claim:
There’s a causal relationship between your thoughts, your feelings, and your actions.
It follows: if you change one factor here, you may be able to change others as well.
Notice that this model, as I’ve construed it, does NOT presuppose (as many CBT™ Manuals will) that the chain of causality always and everywhere runs from thoughts to feelings. Indeed, one of CBT™’s original sins is that it put so much emphasis on this one causal pathway to the exclusion of the others. But in reality, it’s clear that every one of these six arrows maps on to the human experience. At the risk of being pedantic, here are six examples:
Thoughts → actions: You think “What if I left the stove on!” so you turn the car around eight miles into your commute.
Thoughts → feelings: You think “I will be alone forever” and then you feel sad and lonely.
Feelings → actions: You experience social anxiety before a party, so you make an excuse to stay home.
Feelings → thoughts: You are overtired and begin having many unrelated self-critical thoughts.
Actions → thoughts: You go for a walk and think “hey, this day might be 5% less bad than yesterday.”
Actions → feelings: You go for a walk and feel 5% less bad.
To be clear, the cognitive model is not the kind of hard-won wisdom you reach after a lifetime of contemplation on the human condition. It’s not a mind-blowing scientific breakthrough worth patenting, trademarking, or giving a TEDx talk about. And it’s certainly not #one-weird-trick to wipe away all tears and misery and suffering from this world.
It’s the opposite. It’s a framework so basic that you can teach it to an 8-year-old in two minutes. It’s something that people already pretty much know. It’s a truism. It’s basic. It’s almost tautological in its simplicity.
As such, it isn’t meant to stand in as a definitive, multidimensional depiction of the human experience. Insofar as clinicians do this in their practice, they err severely, erasing their clients’ subjectivity and providing the kind of 1D therapy that you’d expect from a chatbot.
So the cognitive model is NOT the pinnacle of effective psychotherapy, or the end of the clinical conversation. It’s just an extremely humble, extremely basic starting point.
It’s the simple, strong, comprehensive-enough bones out of which the skeleton of a working case conceptualization can be formed. For non-therapist readers, “case conceptualization,” is just a therapist’s working model of what might be causing and sustaining their client’s suffering, and what it might take to break those cycles.
Out of the basic building blocks of the cognitive model, we can construct a more elaborate and personalized skeleton frame of the clinical picture. For instance, here is a (fictitious) case conceptualization for a person struggling with, among other things, disordered eating patterns:
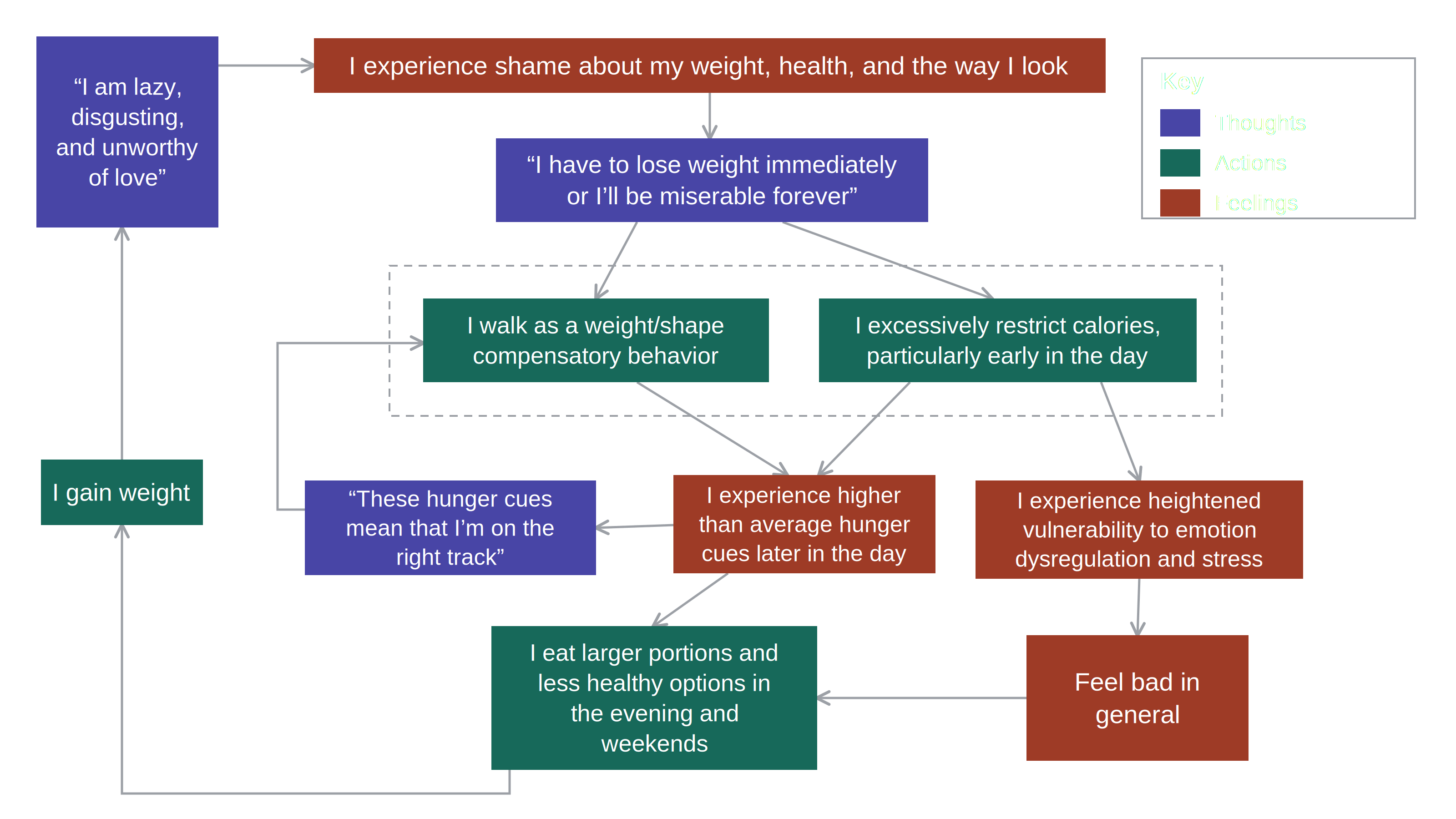
You can see how this might be useful. In this case, many possible paths jump out, including (but not at all limited to):
Focusing on the belief that hunger means they’re “on the right track.”
Building non-food methods of handling stress and difficult emotions.
Working directly with the shame and themes related to self-worth and love.
Establishing regularly scheduled eating across the day.
What specific paths to take will depend on the particularities of the client and where they are both in treatment and in their lives. A one-size-fits-all approach wouldn’t be helpful to provide, and nor would a one-size-fits-all case conceptualization. Instead, this is something that you can build for every client, possibly collaboratively, and iteratively over the course of therapy. And just like the cognitive model, this case conceptualization is NOT supposed to stand in as a full and comprehensive picture of the client’s lived experience; it’s a map, not the territory. The point is that the model is simple enough for therapist and client to grok in minutes, but extensible enough to map a wide range of psychological issues you’ll see in practice.
So let cbt’s cognitive model be nothing more than the bones of treatment, and the case conceptualization be nothing more than the skeleton. All the rest of the craft—the way that you interact with your client, the way you approach them in all their humanity—can be the muscles and sinews and soft tissues of therapy; the parts that jump out as truly person-specific and truly unique. Good clinicians can differ vastly in their style, and cbt, as I see it, shouldn’t be in the business of monitoring the intricacies of interpersonal relating, of forming working alliances, of eliciting a client’s buy-in, of holding space for suffering and hope and the full panoply of the human condition.
I think this is what John Norcross was getting at when he advocated that we need a different therapy for every individual. And the underlying core of cbt not only allows for that; it practically begs for that.
IV. cbt as a Therapeutic Lingua Franca
Perhaps the most useful aspect of the cognitive model isn’t what it includes but what it leaves out. This model takes pretty much no stand on the things therapists fight about all the time. It won’t tell you which way the causal arrows are pointing in a particular case, or which dynamic process is the best to target, or how far back the chain of causality runs, either in developmental, cultural, or evolutionary terms.
That theoretical thinness is generally seen as a weakness, but it’s precisely that thinness that lets the cognitive model serve as a common notation—a lingua franca or Rosetta Stone into which richer but otherwise mutually unintelligible therapeutic traditions and orientations can be translated, conceptualized, and usefully compared.
Spend any time in clinical circles and you’ll realize that therapists of differing orientations are often awash in their respective jargons and run the risk of talking past each other. In this milieu, many early career therapists feel completely adrift; there’s a gnawing sense of imposter syndrome that comes along with all of this orientation-specific verbiage. Ironically, CBT™ as an orientation is perhaps the greatest contemporary purveyor of overly-complicated jargon (e.g., using terms like “cognitive distortion,” “behavioral activation,” and “cognitive restructuring” instead of “bias”, “doing fun things,” and “thinking differently”).
Jargon has also been a particularly pernicious issue in the psychodynamic tradition, though there have recently been effective efforts to counteract this. This is real progress, and I submit that the cognitive model can do similar work across the entire panoply of psychotherapies.
For instance, watch how much the cognitive model can absorb:
Take Evolutionary theory, which supplies some of the why that the cognitive model leaves blank. It does so by clarifying that the belief, feeling, and action nodes all come pre-loaded in advance by natural and sexual selection. The threat-detection that fires in anxiety and the social-defeat routine that fires in depression are priors installed by selection rather than learned from your particular life. In the notation that relocates the lever: if what looks like a distortion is an adaptive default misfiring in a novel environment, then disputing it as a thinking error will often whiff, and the better move is to change the situation input so the loop stops getting triggered (e.g., touch grass; hug and be hugged; deadlift; feed, water, and walk your human animal). Evolutionary theory provides a full case-conceptualization, but it can build from the bones of the cognitive model.
Or take Attachment theory, which fills in how far back different beliefs got set and rendered into thought-feeling-action loops in the context of intimate relationships. In intimate interpersonal situations, certain beliefs will arise (”they’ll leave,” “they’ll engulf me,” “they’ll love me”) that were laid down in early development by caregivers; the response you pull from the other person tends to confirm the belief that produced it. Run that same thought-feeling-action loops a few thousand times from childhood and you get an attachment style—something nonetheless describable in terms of the cognitive model.
Emotion-focused therapy doesn’t have to reject the cognitive model either; these practitioners just emphasize different arrows, treating emotion as an important source of information rather than a consequence of “biased” thinking. Put in terms of the cognitive model, maybe there are important insights to be gained from examining one’s specific emotional state and how that impacts thoughts and behaviors.
Heck, even relationally-oriented psychodynamic work becomes legible in terms of the cognitive model. A recurring interpersonal pattern that repeats itself in therapy can be usefully construed as a set of beliefs, actions, and feelings that all interact to maintain each other over and over again. Here, the technique of analyzing the transference can be recast as interrupting the automaticity of those thought-action-feeling loop, creating space for reflection and, ultimately, for alternative responses.
None of these orientations, theories, or therapy techniques are wholly reducible to the cognitive model. They wouldn’t be worth much if they could be. But they can all be recast through the lens of the cognitive model to become more universally intelligible for other therapists and broader audiences. Think of the cognitive model as merely the shared coordinate system, a basic map that lets a therapist trained in one tradition understand what a therapist trained in another is actually saying.
Taking a step back, I’d submit even that thinking in broadly cbt terms is what most effective providers already do, even the ones who don’t call themselves cbt therapists, even the ones who write posts dunking on cbt. They investigate a client’s challenges, look into their patterns of thinking, feeling, and acting in the full context of their clients’ lives, build a real human relationship, and then use this relationship as the shared ground on which to help their client make progress on the issues that matter to them.
…So there it is—the strongest possible rehabilitation of cbt that I am able to give. I’m not sure how well it all holds together, but after all that time I spent reading those Treatments That Work manuals, I truly hope it’s something. And even if the above is nothing more than a subtle way of expanding cbt to encompass other therapeutic orientations that I gravitate towards more naturally, perhaps that’s enough. After all, I’m not the first clinical trainee who's had to deal with CBT™ hegemony, and I certainly won’t be the last. Your mileage may vary.
V. Conclusion
Cognitive behavioral therapy is sometimes presented as the only good form of therapy out there, and other times as nothing but false advertising and positive thinking. But for all the ink that’s been spilled on this issue, I think the problem may actually soon be going away on its own. For one, the foibles and failings of CBT™ are evident to anyone capable of critical thought, and bad therapy just won’t hold up in an increasingly therapy-literate marketplace of treatment seekers.
Moreover, I predict this entire style of cookie-cutter, manualized, worksheet-based therapy will be replaced in the next decade or so by therapy chatbots. The snake of clinical science is already eating its own tail, and most of the energy in treatment development is going towards low-touch digital interventions. This will not be the end of psychotherapy as such, but it will mark the demise of CBT™. If chatbots can have people fill out those worksheets faster/better/cheaper, so much the better.
Accordingly, perhaps the therapist community (myself included) could stand to focus their attention on something other than the unbearable lameness of CBT™.
Because we have a lot of issues across the mental health landscape.
We have therapists sleeping with clients. We have therapists still practicing past-life regression therapy. We have the promise and perils of newly emerging psychedelic-assisted therapies. We have charismatic internet wellness gurus promising healing for nine easy payments of $99.99. We have thousands of people not on psychotropic medications who should be. And we have millions of people on psychotropic medications who shouldn’t be.
There are a lot of battles worth fighting; at this point, beating up on CBT™ feels a bit like bullying the science fair whiz kid. Yes, he’s lame. But he’s also smart, and inarguably right sometimes. So let’s make as much use of his gadgets and gizmos as we can, leveraging all the best to help our clients, and finally setting aside all the rest.
…Including the Truly Abysmal Aesthetics:

(Wampold & Imel, 2015). One nuance here is that fewer therapies than you might think have ever even gone through an open-label pilot trial.
E.g., Exposure and Response Prevention (ERP), Prolonged Exposure (PE), Cognitive Processing Therapy (CPT), Dialectical Behavior Therapy (DBT). Sidenote: clinical science uses acronyms to make itself seem more like the biomedical sciences, but I think the only people we reliably impress are each other.
…and because there was some small, alien part of me that thought “maybe put the ego aside this one time and try your best to be teachable.” 2/10, would not recommend.
I appreciate the framing of Lingua Franca and thinness. I wish I had more fully formed thoughts to give back to that, but I wonder if there’s any relationship between that and the on-its-face experience-distant feeling of CBT. When I was younger and first thinking about getting therapy for myself, and was an obnoxiously scientistic “rationalist” who would have been proud of my alexithymia if I could read, CBT seemed like the thing I wanted both because it had the evidence base and because it could work at the level of something I was aware of and comfortable with (thoughts). Now, I strongly believe that most clinicians and trainers involved in it are more open and human than that caricature I’m making of myself, but there’s still a part of me that wonders if the bad aesthetics are (or at least were in the 90s) appealing because they felt appropriately rational for a therapy at the End of History.
Something else I’m still trying to parse out in all this: why doesn’t goal agreement ever show up as a common factors difference that therapeutic models would weigh on? It’s hard for me to imagine that treatment plans formulated and communicated in line with CBT, Shedler-style modern psychodynamic, IFS and whatever else are all equally believable, meaningful and helpful for guiding concrete action for clients. It’s possible I’m heavily overintepreting what Wampold meant by goal agreement as I’m writing that, but it’s on my mind to go back and read him to find out.
I have never felt more seen about why and how I use cbt. Also, your point about where we could point our focus of concern is dead on. Great article!